
Neck pain in children is not an uncommon presenting complaint in a paediatric accident and emergency department. Sheffield has a population of approximately 97 000 children of whom 33 874 attended the accident and emergency department at the children’s hospital in a one year period from 1998 to 1999. Of these, about 817 had pain in the neck region as part of their presenting complaint.
Neck pain in adults is often a manifestation of degenerative disease of the spine whereas in children the commonest causes are trauma and infections. There are other less common but more sinister underlying causes of neck pain. The aim of this paper is to highlight these unusual conditions which present as neck pain.
Most junior doctors term muscular spasm in the neck region as torticollis. Not all kinds of unusual neck posturing and pain, however, are due to torticollis and not all cases of torticollis are benign.1,2 This differentiation is important in the clinical work up of these patients.
We describe five patients who attended the accident and emergency department at our hospital with a presenting complaint of neck pain. These cases highlight the importance of careful evaluation of neck pain in children to prevent delay in diagnosis of less common but more serious underlying conditions. The clinical features in the history and/or examination which should raise suspicion of a less benign cause of the neck pain are highlighted with an asterix (*).
CASES
Patient 1
A 6 year old boy presented with neck pain of sudden onset and restricted neck movement. He was unable to localise the exact site of the pain. There was no history of trauma, systemic upset, or any neurological symptoms prior to the onset of the pain. On examination he held his neck flexed and had restriction of all movements. Systemic examination including neurological examination revealed normal findings. An initial diagnosis of torticollis due to muscle spasm was made. On review in the orthopaedic clinic four days later, his neck pain had worsened* and he held his neck fixed in hyperflexion such that his chin was touching the chest*. Clinical examination was unremarkable except for the abnormal neck posture. Plain x rays of the cervical spine showed normal findings. A magnetic resonance imaging (MRI) scan revealed a large intramedullary tumour in the cervical and upper thoracic region from C1 to T2 (fig 1).

T1-weighted MRI scan of the cervical spine showing a large intramedullary tumour in the cervical and upper thoracic region C1–C5.
Patient 2
A 5 year old child presented with general malaise and neck and back pain of two days’ duration. Initial examination revealed neck tilt to the left and a kyphotic posture of his upper torso. He responded to ibuprofen and though the abnormal neck posture persisted he could straighten his back. A presumptive diagnosis of torticollis due to muscle spasm was made and a review appointment arranged in four days time. On this visit he appeared visibly distressed* with a pain score of 8/10 (1 = pain free; 10 = most painful) and anxious and had a pronounced stoop with hips held in flexion and neck tilted to the left*. He refused to flex his neck but rotated it laterally. Initial investigations including full blood count, C-reactive protein and x rays of cervical and thoracolumbar spine revealed normal findings. Further imaging including an ultrasound scan of the abdomen and computed tomography (CT) scan of cervical spine also had normal findings. An MRI scan of cervical spine showed discitis involving C6/C7 disc (fig 2).

T1-weighted MRI scan of the cervical spine showing discitis involving C6/C7 disc.
Patient 3
A 2 year old boy presented with symptoms of upper respiratory tract infection and pain in his neck. No obvious cause of this could be identified, that is inflamed pharynx or tonsillitis. In view of his young age* at presentation and no obvious cause for the pain identified on preliminary investigation (plain x ray head and neck), further investigations were arranged. A CT scan of head and neck showed marked abnormality of the posterior aspect of base of skull with abnormal fusion of the posterior aspect of the foramen magnum. He was referred to neurosurgery and an MRI scan showed complex abnormality of craniocervical junction with a possible cranium bifidum (fig 3). The child had by now started complaining of headaches of increasing frequency and severity. Currently he is under regular follow up with the option of surgical intervention should this be indicated.

T1-weighted MRI scan of the brain and craniocervical junction showing a Chiari-type malformation.
Patient 4
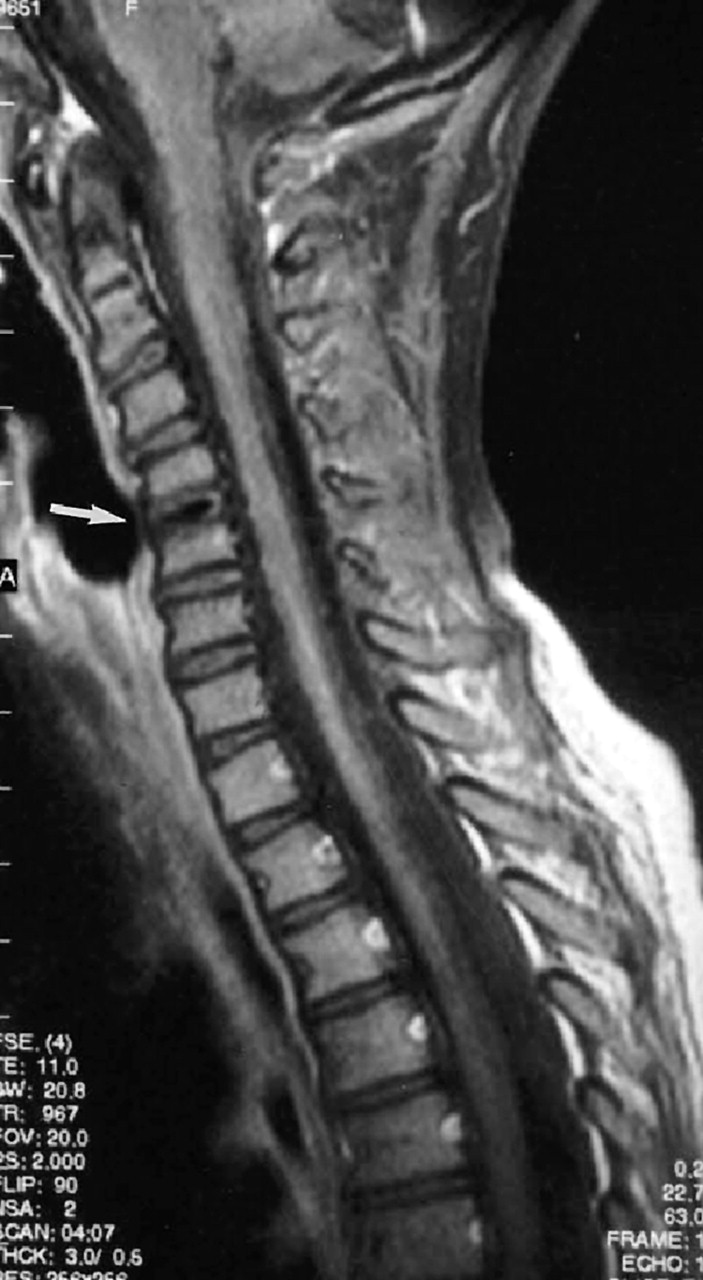
A 4 year old girl presented with a history of intermittent neck pain since a few months. Previous episodes had settled spontaneously without any treatment and she had not been referred to the hospital. On this occasion the pain had commenced on waking* in the morning and lasted through most of the day*. There was no history of recent or past trauma and she was otherwise fit and well, with no obvious cause for the pain. On examination, there was nothing abnormal other than mild stiffness of the neck. She had a full range of neck movements and no abnormal neck posturing. Due to the recurring* nature of the pain and its spontaneous onset on waking*, it was felt that baseline investigations should be done. Plain radiographs of the cervical spine showed unusual calcification at C4–C5 disc level (this is an unusual but well recognised cause of neck pain in children, with 70% of the calcifications seen in the cervical region. The aetiology of this in children is unknown and patients typically present with pain, decreased range of movements and torticollis). An MRI scan confirmed this to be intradiscal calcification (fig 4). Her symptoms settled with non-steroidal anti-inflammatory drugs.

T2-weighted cervical spine MRI scan showing calcification of intervertebral disc between C4 and C5 (arrow).
Patient 5
An 8 year old child presented with neck pain and restriction of terminal neck movement, predominantly rotation. She had a history of intermittent neck pain for the past two years, which had been ignored by the parents. On this occasion however the pain was more acute in onset and of an increased intensity*. Once again, as in patient 4, due to the recurring* nature of the pain, its increasing intensity, and no obvious cause elucidated from either the history or the examination, further investigations were requested. Blood tests including rheumatological profile were normal. Cervical spine anteroposterior and lateral views showed normal findings. An open mouth view x ray of the cervical spine showed osteophyte-like excrescence at the C1–C2 articulation (fig 5) suggesting a possible enthesopathy. Symptoms persisted but with no systemic or joint involvement. A rheumatology opinion was requested but no confirmatory diagnosis has been made. We presume her symptoms are related to the abnormal articulation or may be an early manifestation of an enthesopathy.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Open mouth view x ray of the cervical spine showing osteophyte-like excrescence at C1–C2 articulation (arrows).
DISCUSSION
Neck pain is a common problem encountered in paediatric accident and emergency departments, requiring exclusion of serious underlying pathology and decisions regarding the extent of work up needed. The pain may or may not be associated with an acquired torticollis. Torticollis (Latin word meaning “twisted neck”) is tilting and rotation of the head to one side with restricted rotation towards the other side. It is a symptom of cervical spine abnormality.1,3–5 Neck pain may be associated with neck deformities such as torticollis, kyphosis, or a shortened neck and/or with symptoms of neurological compromise and systemic illness.4 The more common causes3,4,6,7 of neck pain include:
infections8,9 (meningitis, pneumonia, otitis media, tonsillitis, cervical adenitis, retropharyngeal abscess, mumps, and cerebral abscess)
trauma
The less common causes include:
juvenile chronic arthritis10
Arnold–Chiari malformations11
posterior fossa and cervical spinal tumours12
vertebral anomalies
cervical osteomyelitis
spondyloarthropathies
myositis ossificans progressiva.
Some conditions presenting with both neck pain and torticollis include trauma, infections, tumours13–15 (spinal cord and head and neck tumours), calcified intravertebral disc16 and Sandifer’s syndrome.17,18
In most patients presenting with neck pain a cause for this is easily identifiable. However, in the few that it is not obvious, follow up and further investigations may be needed to reach a diagnosis. We suggest that a detailed history covering the points listed in box 1 should be taken from all children presenting with neck pain. Presence of any of these features either in the history or on clinical examination should act as a warning sign for further investigation and or follow up of these patients to help differentiate between a benign and more sinister cause of the neck pain.
Box 1: Neck pain. Points to cover in history and examination
Time of onset of pain (spontaneous onset at night or night pain)
Any associated trauma
Any relieving or exacerbating factors
Pain in the occipital condyle (seen in posterior fossa tumours)
Score the pain on available pain charts
Duration of pain, whether continuous or intermittent
Interference with daily activity
Any history of drugs especially those causing extrapyramidal side effects
Problems with vision
Other associated symptoms like headaches, vertigo, vomiting
Unusual neck posturing, that is, hyperflexed position, child trying to splint the neck with their hands. These should raise the suspicion of posterior fossa tumours, discitis and spinal cord tumours
Any gait abnormalities (base of skull tumour and spinal cord tumours) and repeated attendances at the hospital with persistence of symptoms
A complete physical examination should include examination of the neurological system, spine, and eyes especially eye movements and the cover–uncover test.7,19 If then an initial diagnosis of muscular spasm is made the child should be asked to return for follow up in 48–72 hours should the pain persist. A second clinical examination may give more clues and more appropriate imaging modalities can be used.
The basis of a proper clinical diagnosis remains the patient’s history and physical examination. Unusual presentation with neck pain, abnormal neck posturing, gait abnormalities and its persistence should ring a warning bell for other potentially less common but more sinister diagnoses. The examiner’s index of suspicion is crucial to the completeness of work up of patients with neck pain with/without torticollis. With easy access to imaging modalities, conditions like intracranial tumours of the base of skull, intraspinal tumours, congenital abnormalities, and spinal infections can be easily diagnosed and early treatment instituted.
This series of unusual and rare case reports highlights that physicians in the paediatric accident and emergency department need more awareness when dealing with children with neck pain and abnormal neck posturing. A search for atypical features of neck pain and abnormal neck posture should avoid delays in diagnosis and appropriate referral and management.
No comments:
Post a Comment