Abstract
Background Little is known about the quantity and reasons for use of palliative sedation in general practice.
Aim To gain more insight into the trends of and reasons for palliative sedation in Dutch general practice.
Design and setting Dynamic cohort study using registrations and questionnaire data of Dutch GPs.
Method Data collected in the years from 2005 until 2011 in the Dutch Sentinel General Practice Network were analysed. Trends and reasons for use of palliative sedation were analysed using multilevel analyses to control for clustering of observations within general practices.
Results From 2005–2011, 183 cases were reported from 56 general practices. The incidence of palliative sedation fluctuated between 33.7 per 100 000 patients in 2006 and 15.2 in 2011. No rise or decline during the period was observed. Palliative sedation was applied in 5.7% of all deaths and most frequently used in younger patients with cancer. The mean number of refractory symptoms was 2.6 (SD 1.2); pain (69.4%), dyspnoea (53.0%), and fear (39.3%). Patient involvement in decision making before the start of palliative sedation (87.4%) was less frequently present in patients suffering from cardiovascular or chronic obstructive pulmonary disease and in older patients compared to patients with cancer (P<0.05). Pending euthanasia requests were present in 20.8% of cases; the choice for palliative sedation in these cases was clearly motivated.
Conclusion Palliative sedation is performed in a small proportion of dying patients in Dutch general practice, without a rise or decline observed from 2005 to 2011. Patients with non-cancer diseases are less frequently involved in decision making than patients with cancer, possibly related to sudden deterioration.
INTRODUCTION
Palliative sedation is defined as intentional sedation in the last phase of life to alleviate intolerable refractory symptoms. Symptoms are refractory if there is no effective treatment, in an acceptable time frame, or if the treatment is intolerable. Palliative sedation includes continuous deep sedation as well as superficial, short, and intermitting sedation, where the goal should not be the loss of consciousness until death but an adequate alleviation of symptoms.1–3 When appropriately indicated and correctly used, palliative sedation does not accelerate death.4–7
Since the introduction of the Dutch national guideline on palliative sedation in 2005 the opinions of the public and of physicians regarding palliative sedation have changed. The familiarity with palliative sedation has increased and the patient is more often, and at an earlier stage, included in the decision making although the treating physician is finally responsible.8 From the guidelines it is clear that palliative sedation is only indicated when imminent natural death is anticipated to occur within 2 weeks. In 2009 a revision of the Dutch national guideline was published which addressed several areas of debate including the compliance with the guideline, the practice of palliative sedation and the relationship to euthanasia.1
Onwuteaka-Philipsen et al described an increase in continuous deep sedation by Dutch GPs, clinical specialists, and nursing home physicians in 2010 (12.3%, 95% confidence interval [CI] = 11.6 to 13.3) compared to 2005 (8.2%, 95% CI = 7.8 to 8.6). However, due to a lack of data from the intervening years it is uncertain if this is an incidental rise or a result of an increasing underlying trend.9 In addition, this study included medical specialists and nursing home physicians. In 2005 clinical specialists were followed by GPs (34%) and nursing home physicians, whereas in 2010 GPs most frequently performed continuous deep sedation (43% of cases).10,11 The refractory symptoms of pain (33%), physical exhaustion (33%), and dyspnoea (24%) were the most common indications for palliative sedation in patients with cancer and pain (22%), physical exhaustion (21%), and dyspnoea (41%) for non-cancer patients.12 National and international studies described palliative sedation to be used more frequently when patients were younger, male, or were dying of cancer and more frequently in a hospital setting.13–17
Previous research has shown a rise in performing palliative sedation; whether or not this rise is applicable in general practice and whether or not this rise is developing into a trend is still unknown.9,10 The aim of this study was to provide a better understanding concerning the practice of palliative sedation in general practice over the course of recent years, describing patient characteristics, the underlying diseases and indications as well as the decision making itself. A further aim was to obtain a better understanding about the reasons for performing palliative sedation in patients with a pending request for euthanasia in general practice. Euthanasia is based on the request of the patient, where palliative sedation is often considered as a primarily physician-based decision in case of refractory symptoms.1,18 It is unknown if the increased familiarity of palliative sedation among the public and among physicians has led to a change in the number of pending requests for euthanasia in the patients who receive palliative sedation. Consultation of the patient or proxies is not always possible but nevertheless desirable. The years following the introduction of the guideline marked an increase in patient involvement.8 Did the introduction of the guideline lead to a sudden change in patient involvement, or has the involvement in the decision making changed more comprehensively? Five research questions were asked:
- Is there a significant trend (increase or decrease) in the incidence of continuous deep palliative sedation in Dutch general practices during the period 2005–2011?
- What is the proportion of continuous deep palliative sedation extrapolated to all deaths in Dutch general practice?
- What are the underlying diseases and symptoms of the patients?
- If there was a pending request for euthanasia why was deep palliative sedation chosen?
- Who is involved in the decision making regarding deep palliative sedation and has there been a change in the period 2005–2011?
How this fits in
Palliative sedation is defined as intentional sedation in the last phase of life to alleviate intolerable refractory symptoms. Palliative sedation is only indicated when imminent natural death is anticipated to occur within 2 weeks. When appropriately indicated and correctly used, palliative sedation does not accelerate death. There was no increasing or declining trend in the incidence of palliative sedation in Dutch general practice during the period 2005–2011. Palliative sedation was most frequently used in younger patients with cancer and with multiple refractory symptoms, predominantly pain, dyspnoea, and fear and was performed in 5.7% of all deceased patients. Patients with non-cancer diseases were less frequently involved in decision making. A clear distinction between performing palliative sedation and euthanasia in Dutch general practice is shown.
METHOD
Retrospective registration and questionnaire data from 2005 through 2011 were derived from GPs participating in the Dutch Sentinel General Practice Network at NIVEL, the Netherlands Institute of Health Services Research. This network, existing since 1970, is nationally representative by sex, age, regional distribution, and by population density, covering about 0.7% of the total Dutch patient population.19 Most practices participate for many years. This network is designed to collect data from electronic medical records (EMRs) in general practice with additional data by questionnaire and/or samples of urine and/or nose and mouth swabs to survey weekly incidence of influenza, whooping cough, sexually transmitted diseases, antibiotic resistance, end-of-life care and other subjects which cannot be studied by EMRs exclusively. Each year a few practices terminate their participation for diverse reasons and are replaced by other practices, that is, a dynamic cohort. In total, 75 general practices participated in the Dutch GP Network in the period between 2005 and 2011, on average 43 practices per year; 56 of these practices reported palliative sedation in this period. For this study, from 2005 GPs were asked to register weekly if palliative sedation was performed and if so a questionnaire with additional questions was sent by postal mail. Reminders were sent at the end of the year at least twice and followed up with telephone calls in case of no response. Palliative sedation was defined as:
‘Continuous deep sedation of a patient, with the use of adequate doses of sedatives, to alleviate severe suffering, without the aim to end life. A life expectancy of no more than 2 weeks is required. Continuous deep sedation can also be applied for a short period of time (24–48 hours) in severe acute conditions’.1
The questionnaire contained the following items: age and sex of the patient, underlying disease, symptoms that were a reason for the deep sedation, whether or not there was a pending request for euthanasia and the persons involved in the decision making. Since 2007 the questionnaire also contained the reason why palliative sedation was performed in case there was a pending request for euthanasia. Diseases were classified using the International Classification of Primary Care system. Questions on symptoms were pre-structured and subdivided by delirium, dyspnoea, pain, nausea, vomiting, fear and other. The persons involved in the decision making were categorised as patient, family, nurses and other physicians.
Statistical analysis
The incidence and proportion of palliative sedation per 100 000 patients in the Dutch general practice population was calculated and stratified by sex to analyse a possible trend (increase or decrease) in the incidence of continuous deep palliative sedation and the proportion of continuous deep palliative sedation extrapolated to all deaths in Dutch general practice during the period 2005–2011. Incidence rates of palliative sedation, diseases and symptoms were calculated using multilevel analyses to control for clustering of observations within practices, including Poisson regression for incidence rates of palliative sedation and logistic regression for incidence rates of diseases and symptoms. This method was chosen to adjust for large interpractice variation and skewed distribution. All participating general practices were included, also practices that had not performed palliative sedation. The time trends were estimated using a second order polynomial (=quadratic variable) for time, to allow for a potential non-linear trend. Indicators were added to the multilevel model to estimate the influence of urbanisation as urbanisation was anticipated to potentially be a predictor of increased use of palliative sedation. Beside these two effects (time trend and urbanisation), the interpractice variation, as estimated by the multilevel model, was used to calculate the 95% coverage interval, the interval supposedly including 95% of the practice averages in the population. The statistical analyses were performed using Stata/SE (version 12.1), multilevel analyses were performed using MLN — Software for N-level analysis.
Descriptive methods were used to address the calculation of the proportion of palliative sedation extrapolated to all deaths, the age distribution compared to all deaths, the underlying diseases and symptoms, the reason to perform palliative sedation in cases with a pending request for euthanasia, the description of who is involved in the decision making and possible trends over time. Logistic regression was used to differentiate between attributing patient characteristics (age, sex, underlying diseases, and practice characteristics) of assorted categorical dependent variables (symptoms, pending euthanasia requests, and consulted persons).
RESULTS
During the study period 2005–2011 a total number of 183 patients who died after palliative sedation was reported by the 75 practices participating in the Sentinel network; 177 in general practice, five in the hospital, and one died before the palliative sedation was initiated. The incidence of palliative sedation per year from 2005 to 2011 fluctuated between 33.7 per 100 000 registered patients in Dutch general practice in 2006 and 15.2 in 2011 (Table 1). The interpractice variation was large, ranging from 3.2 to 68.7 cases of palliative sedation per GP per 100 000 registered patients. It is important to notice that this interval can be much wider than the CI around the general average or the difference between urbanisation classes (Figure 1). This would mean that a large interpractice variation is observed and not explained by the factors in the model. Palliative sedation accounted for 5.7% of all deaths in Dutch general practice during the study period (Table 1). There appeared to be no significant trend in the incidence of palliative sedation overall in this study period by logistic regression (P = 0.39) and by multilevel analyses (P = 0.35) (Figure 1). Palliative sedation was not related to sex (P = 0.127). The mean age of patients was 71 years (range 39–100 years, standard deviation [SD] 13.6). Palliative sedation was relatively more frequently performed in the age group ≤74 years as compared to older age groups when a comparison was made with all deaths reported in the same network in the same period (Table 1, P<0.01). Population density was not associated with the incidence of palliative sedation as shown by multilevel analyses.
Table 1
Characteristics of patients receiving palliative sedation (n = 183) and refractory symptoms in Dutch general practice, compared to age distribution of all deceased 2005–2011
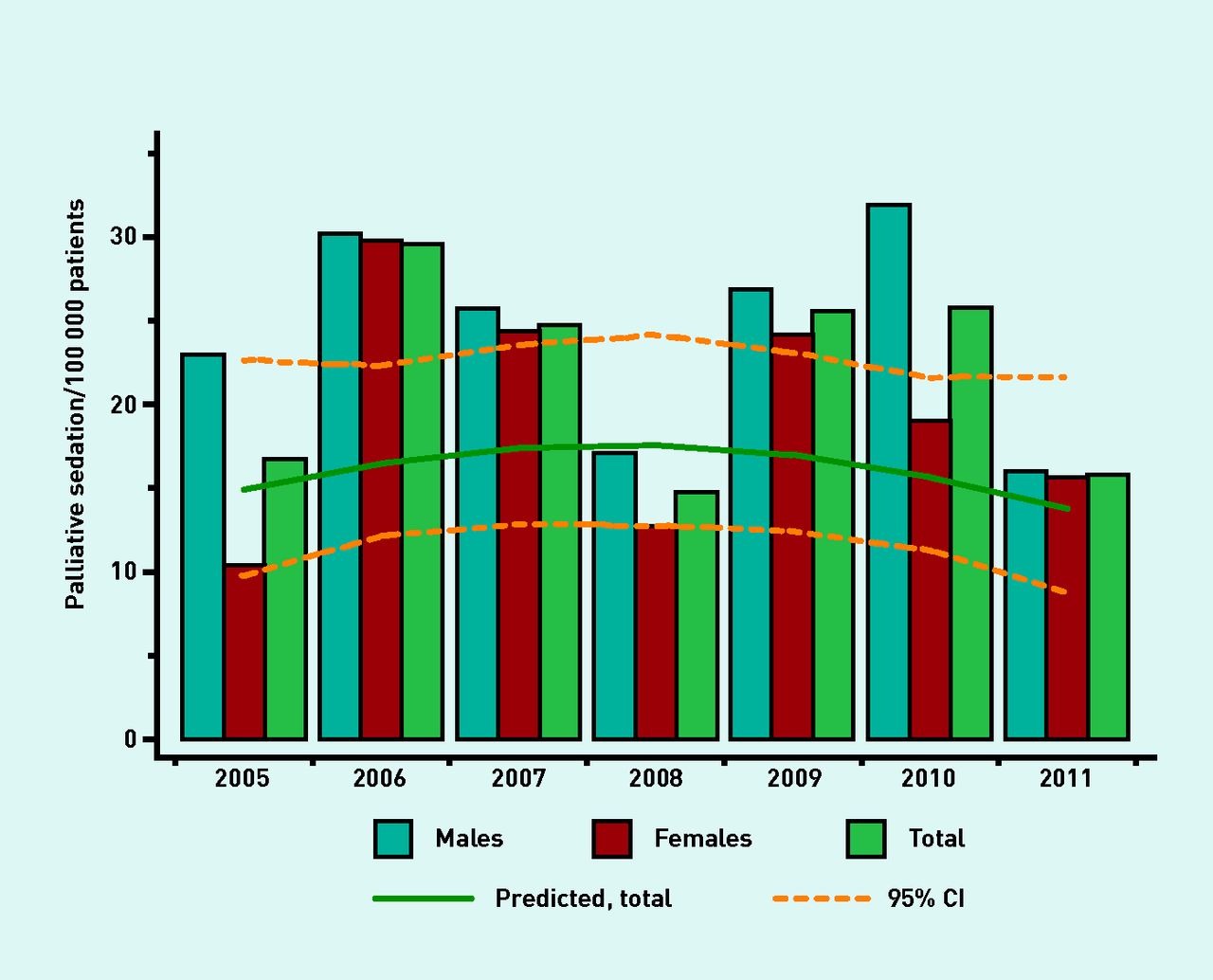
Figure 1
Trends in incidence of palliative sedation in Dutch general practice per 100 000 by sex and total, 2005–2011. Weighted using multilevel Poisson regression analyses for sampling fractions and population density. Trends are visualised using multilevel Poisson regression analyses with grade-2 polynomal (=quadratic) trend lines.
Underlying diseases
The most frequently reported underlying disease was cancer (73.8%) (Table 1), which was more often present in patients ≤64 years (P = 0.008). Cardiovascular and chronic obstructive pulmonary disease (COPD) composed a smaller group (8.7% and 3.8%). Other diseases (including dementia, frailty and neurologic disorders) constituted 18.0% of the patients. Patients with cardiovascular or other unclassified diseases were significantly older (P = 0.001). Trends over years in the underlying diseases proved not to be statistically significant, as confirmed by multilevel analyses.
Refractory symptoms
Pain was the most reported refractory symptom (69.4%), followed by dyspnoea (53.0%) and fear (39.3%) (Table 1). Nausea and vomiting were present 29.5% and 24.6% respectively, the sum of these incidences was 39.3%. Nausea was significantly more often present in patients aged ≤64 years (P = 0.043) or with cancer (P= 0.002). Vomiting was also significantly related to a younger age (P = 0.014) and cancer (P = 0.028). Delirium (24.0%) and ‘other’ symptoms (24.8%) composed the smallest group. Other symptoms mentioned were: exhaustion (n = 9), cachexia (n = 8) and dysphagia (n = 3). Delirium was more common in regions with low population density (<500/km2) than in urban areas (P<0.001 for 500–2500/km2, P = 0.032 for >2500/km2). Trends in the refractory symptoms proved not to be statistically significant, as confirmed by multilevel analyses (Figure 2). The majority of patients suffered from multiple symptoms, the mean number of symptoms was 2.6 (SD 1.2).

{kind=link}
{kind=link}
Figure 2
Trends in indications for palliative sedation in Dutch general practice, 2005–2011, percentages with a specific refractory symptom. Weighted using multilevel logistic regression analyses for sampling fractions, population density, age, and sex. No data was collected of ‘other symptoms’ in 2005 and 2006, ‘other symptoms’ are not weighted for population density. Trends are visualised using multilevel logistic regression analyses with grade-2 polynomal (=quadratic) trend lines.
Pending euthanasia requests
Pending euthanasia requests were present in 20.8% of the cases, ranging from 10.0% to 31.3% (Table 2). The reasons reported for not performing euthanasia could be classified as ‘short life expectancy or rapid progression’, ‘incomplete euthanasia request’, ‘impaired cognition or speech’, ‘patient’s wish’, ‘organisational or procedure problems’, ‘family’s wish’ and other. Patients from the western provinces of the Netherlands had more often a pending euthanasia request (P = 0.027), there was no association with population density.
Table 2
Characteristics of euthanasia requests of patients who receive palliative sedation in Dutch general practice, 2005–2011
Decision making
Relatives (94.5%) and patients (87.4%) were most frequently consulted about the decision to use palliative sedation, although nurses (54.1%) and other physicians (29.5%) also were involved in the decision making relatively frequently (Table 3). The proportions of consulted patients, relatives, nurses, and other physicians did not change during this research period. Consultation with either the patient or relatives was done in nearly all cases (97.3%). Palliative sedation was most frequently discussed with patients with cancer (90.4%), and less frequently discussed with patients with cardiovascular (75.0%, P = 0.039), COPD (57.1%, P = 0.014) or other unclassified diseases (75,8%, P = 0.012) and older patients (P = 0.008).
Table 3
Persons consulted in the decision making of palliative sedation in Dutch general practice, 2005–2011
DISCUSSION
This study shows no significant increasing or decreasing trend in the incidence of palliative sedation in Dutch general practice from 2005 to 2011. In 2011 13.4 per 100 000 patients in Dutch general practice underwent palliative sedation. Palliative sedation was most frequently used in younger patients with cancer and with multiple refractory symptoms predominantly pain, dyspnoea and fear. Palliative sedation was performed in 5.7% of deceased patients in general practice in this study. An average of one in every five patients had a pending euthanasia request. Reasons for performing palliative sedation when a euthanasia request was present were rapid progress of disease, preference for palliative sedation of the patient and/or family, or an incomplete euthanasia request. The decision to use palliative sedation was discussed in nearly all cases with the patient or family during the whole study period. However, patients with non-cancer diseases were less frequently involved in decision making on palliative sedation than patients with cancer, possibly related to sudden deterioration.
Strengths and limitations
The Dutch sentinel GP network used in this study is nationally representative for the Dutch general practice population, which is a major strength. The study is representative for the average Dutch general practice patient population, especially due to the multilevel Poisson analysis techniques used with adjustment for age, sex, interpractice variation, skewed distribution, and population density. The limited number of cases could have influenced the fluctuation between years in the study, especially in the trends of refractory symptoms and underlying diseases. However, the multilevel analyses and Poisson regression used adjust for the large interpractice variation and skewed distribution. The study cannot directly be compared to other studies not applying multilevel techniques as the adjustment for skewed distribution decreases mean levels. In addition, the study results cannot be extrapolated to the general population as about 14% of people aged >80 years in the Netherlands reside in nursing homes, which are served by elderly care physicians.20 Palliative sedation is used frequently by clinical specialists and elderly care physicians.10,21 A national study reports palliative sedation applied in 12.3% of all deaths in the over-all Dutch population, considerably higher than in the current study.9 Another strength is the use of a long-time existing sentinel network, reducing the chance of a non-responder bias.22 No data were collected about cases where palliative sedation was considered but not performed. However previous research did not find any major differences between groups where palliative sedation was considered but not performed.23
The total number of euthanasia requests in this study could be an overestimation given the fact that incomplete euthanasia requests were among the reasons for not performing euthanasia. Thus, it is not clear if the reported requests were one-time only mentioned options of the patient or long-term sustaining requests. This discrepancy is also present in other large scale studies concerning the incidence of euthanasia and euthanasia requests.10 A recent study reported 45% of euthanasia requests to be carried out.24 The total number of euthanasia requests in the current sample is small, but nevertheless important enough to be analysed as it was not possible to confirm an overlap between euthanasia and palliative sedation as suggested in some international studies.13,17
Comparison with existing literature
The absence of an increasing trend is in contrast with Onwuteaka-Philipsen’s study describing such a trend.11 This could be explained by differences in study design. Previous studies did not investigate deaths over consecutive years as a dynamic cohort study, but had a cross-sectional design comparing two points in time with a wider time gap.9 Other studies reported a slight but not statistically significant preference of palliative sedation in males which could not be confirmed in the current study.10,25 This study shows that three in four patients have cancer and the other quarter have cardiovascular disease, COPD, and other unclassified diseases, a distribution comparable to other Dutch studies.10,25 The finding of applying palliative sedation more frequently in patients of relatively young age and with cancer was confirmed in several national and international studies.15–17
The most frequently reported refractory symptoms in this study (pain, dyspnoea and fear) are different from other Dutch and international studies; the incidence of fear in the current study is higher than in literature.12,26 In contrast, the incidence of physical exhaustion is a major indication in literature and was only a small proportion in this study.12 This could be caused by a difference in the structure and content of the questionnaire items: physical exhaustion was not predefined in the questionnaire of this study but could be reported in an open question. In this study a larger proportion of the patients appeared to be experiencing the most reported refractory symptoms, possibly providing a reflection of the symptom burden in the last week of life.27
Euthanasia is fundamentally different from palliative sedation. Dutch law defines euthanasia as the ending of life of a patient, at their explicit request due to unbearable and lasting suffering, performed by a physician who fulfils strictly-defined requirements.28 The basis of euthanasia is the request of the patient to end his or her life, in contrast to palliative sedation which is medical care offered by a physician to alleviate refractory symptoms. In routine medical practice an informed consent discussion should take place before the start of palliative sedation to explain the procedure and the consequences for patient’s carers. Palliative sedation is recognised as standard medical care in case of refractory symptoms by various guidelines, where euthanasia is an exceptional medical procedure and will never be included in the standard care offered by physicians.1–3,18 The reasons reported for performing palliative sedation in this study in cases with also a euthanasia request are in line with a previous study among Dutch physicians reporting that in 30% of patients with a euthanasia request which was not carried out continuous deep sedation was used.10 In the proportion of patients (one in five) where euthanasia as an option had also been discussed, the choice for palliative sedation was clearly motivated as a final preference of the patient or family, or by the inability to perform euthanasia in a legal way due to rapid progression of symptoms, and inability to communicate with the patient and/or to determine eligibility. This study did not show any indication of a vague border between euthanasia and palliative sedation.
The decision to perform palliative sedation was most frequently discussed with patients with cancer and less frequently discussed with patients with non-cancer conditions. This difference between patient groups could be related to the different disease trajectories as described by Lynn and Adamson.29 The cancer disease trajectory is relatively predictable and death can be relatively well foreseen. In contrast, chronic heart and lung failure is often characterised by intermittent exacerbations and sudden deterioration and death. In addition, the incidence of chronic heart and lung failure is higher in the oldest old who often experience a general physical and cognitive decline which may hamper involvement in decision making in the final phase. Particularly for these patients, timely discussion of care and treatment options, also named advance care planning, is recommended. In these discussions concerning patients’ preferences for future care patients’ thoughts about palliative sedation in case of refractory symptoms in the final phase of life could also be explored.1–3,24,28
Implications for research and practice
Palliative sedation is practised in a small proportion of patients in Dutch general practice and no significant increasing or decreasing trend in the period 2005–2011 has been observed. Recent guidelines for palliative sedation have supported physicians in professionalising palliative care and in performing palliative sedation as a best practice under clearly defined conditions.1–3,18However, timely discussion of options, especially in patients suffering from chronic respiratory and cardiovascular diseases, needs attention.
No comments:
Post a Comment